
english version of my research regarding Methadone, a tool in our toolbox conquering cancer. This article is written for my US-Friends.
Discovery of a useful side effect of Methadone
Dr. Hilscher is a GP in Iserslohe, Germany. He used to guide three hospices. Actually I never talked to him personally but I can easy imagine how they started to use Methadone as a regular pain medication in one of the hospices:
Here in Austria only licenced nurses are allowed to give s.c. injections, but licenced nurses are expensive so old folks homes or hospices usually do have only unlicenced or volunteers in their night shift. If the (dying) inmate / patient has need for a strong pain killer and is not able to swallow, the doctor has to drive in to give the injection himself. Nice next day in a crowded praxis!
We all are tought in our pallliativ care exames (I am a licenced palliativ care physician) that opioids are interchangeable and that actually you ought to exchange opioids regularely to prevent side effects. To do that the physicians are using Conversion-Tables and Calculators like e.g. here.
So Dr. Hilscher was seeking some strong opioid that could be used orally with little side effects and an easy mode of dosing and found METHADONE to be such an opioid.
The 1% solution (consisting of the racemate has actually 0.5% Levomethadone which is the real pain killer) can be applied orally also to unconscious patients, it is resorbed transorally, the action is quite fast (within 5-15 Minutes) and it is very long lasting in its pain-mitigating action: 12 – 48h, furthermore Methadone is removed via liver as well as kidney pathway so that you dont have to have any restrictions of one of the organs (liver metastasis) dont work accordingly.
In the dosages used for cancer patients – usually up to 30mg daily dose – there are basically no side effects other than constipation – only the high dosages used for drug-user heroin replacement you have to consider cardiac action (elongation of QT-interval).
funny enough, in one hospice the patients stopped dying
this is what Dr. Hilscher told on TV: they used Methadone as pain-medication in one of his 3 hospices and there they saw it again and again: patients went back home and lived much longer than what was expected.
It took them some time to attribute that to some influence of Methadone on the Cancer:
Methadone also acts via the µ-kappa-endorphine receptors and they are known since the 70th as being tumorstatic receptors.
Following the Low Dose Naltrexone Connection
Since the groundbraking work of the late NY State Health Secretary Dr. Bihari in the 80th (see interview) we are using Low Dose Naltrexone to stimulate the Endorphine Receptors which slows down the growth of cancers.
Endorphines control 80% of Cancer Growth
from the groundbreaking work of the biochemist Dr. Zagon we know that high endorphines slow down cancer growth by 40% while low endorphines increase cancer growth by 40%.
Methadone is capeable of simulating high Endorphine levels and thus slows down cancer growth which was accidentially discovered by Dr. Hilscher.
Heroin – the ultimate Cancer treatment?
now what is the best of all Endorphines available – yes – its Heroin: you take it once and are hooked because it simulates heaven!
Is there any proof that Zagon / Biharis discoveries regarding Endorphines could be seen with heroin?
2321 Heroin users died for whatever reasons in greek – NON of them developed cancer (study 2016), so the authors of the study desperately seek to understand what is happening, why we “non heroin addicted” develop 50% cancer over live-time and in comparison the “livelong heroin-addicted” stay completely cancer free? (Study 2017).
Actually already Zagon and Bihari cite this phenomenon and traced it to the cancer-inhibiting action of the endorphine receptor.
So lets sum up the first benefit of Methadone as cancer-pain medication
Methadone is an effective opioid medication, around 7 times stronger that morphium in its analgetic action.
Methadone has a remarkable low degree of side effects, this is why we are using it as heroin replacement for addicted people: they get their daily dose of 100-300mg for 30 years without any organ damage
Methadone also acts via Endorphine receptors – in comparison to most of the other opioids – and thus shows some of the “Heroin / LDN” Effect: cancer grows slower.
It still grows – just a bit slower!
Methadone is cleared from our system via kidney and liver, so there are no restrictions if one of the organs have reduced functionality.
Methadone acts quite fast, orally applied and has a very long mode of action: 12-48h – so one could apply it once per day. We have found that the least side effects are when applying it twice per day.
The story of the US-teacher
 Some german biochemist named Dr. Claudia Friesen was working with cancer cells and opioids. She could show that Methadone alone (among all opioids tested) would kill cancer cells in the test tube.
Some german biochemist named Dr. Claudia Friesen was working with cancer cells and opioids. She could show that Methadone alone (among all opioids tested) would kill cancer cells in the test tube.
Later she could show in the mouse model that Methadone would slow down the growth of the cancer, but in such high dosages that are unrealistic for being used in man.
Dr. Friesen told me a story when I met here in Vienna 2017 at the IGMED Meeting:
she was getting an email from the US from some teacher who suffered advanced lung cancer. He was told by his physician he just would live some more weeks and as he had no relatives he sold everything and moved to a hospice. He got Methadone as pain killer from his physician. After a year he had to move out of the hospice because he didnt look dying soon, so he went back to his physician and both were astonished to find the cancer shrunk to a third in sice. As he was free of pain he also stopped his pain medication. His Cancer grew again, he needed pain medication, cancer shrank, he stopped pain medication. This happened 4 times until they realized that the cancer-stopping effect must be attributed to the methadone. So the guy – being a retired biology teacher – looked up the pubmed if there is any explanation and only found Dr. Claudia Friesens work citing the cancer-stopping action of Methadone. So he was writing to Dr. Friesen “Claudia, you have discovered why I am still alive ….”
Dr. Friesen told me, that she was receiving his medical records yearly over 12 years until he finally stopped writing her, probably he died. She does not know anything else about his supposed death (because he has no relative, she does not know whome to ask).
Chemo-adjuvant action of methadone
a Patient XX suffering relaps of his glioblastoma and he got Methadone from me (Dr. Retzek).
When I give patients Methadone I do not tell them that they can expect cure or anything else “miraculous”, I tell them that in the best case they might have a slowing down of their cancer progression, “in the best case you get some extra time”, not more.
To get more out of Methadone they need some cancer destructive therapy, e.g. Chemotherapy or Radiatio together with higher doses of Methadone that sure have quite some side effects: dizzyness, sleepyness, constipation.
I show them that Methadone acts as some kind of Chemo-Support:
only in higher methadone dosage (2 x 20 drops, best 2 x 35 drops = 2 x 17,5 mg daily dose) a bad bad protein named MDR (“multi drug resistancy”) is turned off by methadone.
This protein is the hallmark of Cancer-Stem-Cells and gives them the ability to withstand Chemo and Radiation. If we could get rid off MDR (=gp120) we could probably cure cancer with Chemotherapy.
Thus higher doses of Methadone increase the effectivity of Chemotherapy. The most effect you get with glioblastomas, though in my praxis I am often amazed about positiv feedback of lung cancer patients using methadone together with chemotherapy.
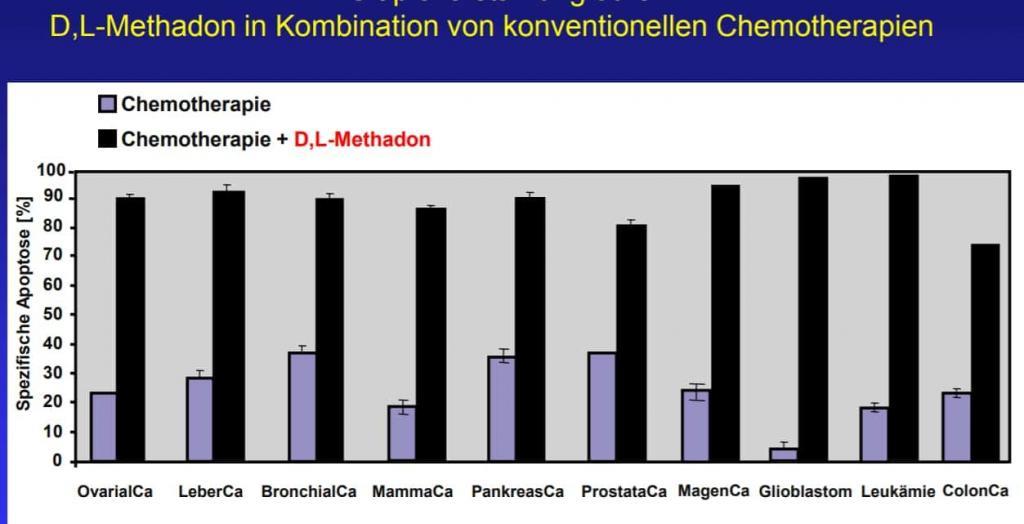
As MDR is the hallmark of any Chemo-Resistancy you get a positive influence of methadone with pretty every tested chemotherapy.
Dr. Friesen went public with her research about 2016 and was overwhelmed with calls from many many cancer patients. She collects cases – which of course is no valid study, just simple observations, but she cites cases where the chemotherapy stopped working until they used methadone as adjuvant and then the same chemotherapy worked again very well.
So I told that my Glioblastoma-Patient XXX: yes, it makes sense to add methadone to your regime. Also add DCA to your daily pills, Dr. Mikelakis in Edmonton could proof 2010 that DCA can inhibit the metabolism of glioblastomas.
The patient told me some months later:
my tumor shrank 50% without any chemotherapy just using 2 x 6 drops methadone and DCA.
My oncologist was totally stunt having never seen anything like that and could not explain it. I did not dare to tell him that I used methadone because when we asked earlier about his opinion regarding methadone he yelled at us like crazy: unproven, does not work, a joke, just use to rip off people by corrupt physicians …..
I admit, this is a special case, I have never seen anything like that having prescribed Methadone to now about 300 patients. One should not use the exeption to feed complete unrealistic hope into patients, still – it happened.
Swiss Cancer Patient is pissed
“hi, I am here again” he said, having visited me many months before. “I have to ride 2000 km to come to you as we have no physicians in switzerland that prescribe methadone to cancer patients”.
“I feel well, I work the whole day, have no pain, everything is good”
“I am now taking 2 x 20 drops methadone a day, having no side effects at all, before I had 400mg of morphium every day, have not been painless and had lots of side effects”
“no, I have no idea whats up with my cancer! Why should I go? They sent me home to die, I am finished they said, I am done, they cannot do anything anymore, so why should I go there again? “
“and Doctor, I have to tell you: my mom is working in drug addiction, so I know what is happening with drug users. They are getting their methadone daily, 200 or even 400 drops per day for free in Switzerland, and no-one says anything or complaints. But if we cancer patients are taking 20 drops and feel well, they would chase us or forbid it? Now you tell me who profits from such a policy, what is up here?”
Regular physicians forbid the use of methadone
soon after the TV Interviews with Dr. Hilscher and Dr. Friesen appeared the professional societies in Germany and Austria wrote statements that methadone as a cancer adjuvans is a hoax.
Now I had seen three talks of Dr. Claudia Friesen since 2015 and found her compelling, serious, honest and convincing. I could not imagine she would make anything up as there is nothing but drawbacks to her: they put all her research money away, she is under immense pressure, bad reputation and has now several law suits (that she all won to my information).
I could expierience the positiv action of low doses of methadone with my cancer sick dad having prostate cancer metastasis in pretty every bone: putting him from Hydromorphone to Methadone was a game changer. The next day he felt improved and we had the impression that the cancer stopped growing. He did 2 years later from his weak heart and dementia, the cancer was not the main issue.
The Methadone Bashing in Austria went so far that patients of mine were getting insulted in the hospital, the oncologists yelling that I should have withdrawn my licence for providing methadone to patients.
Yet my policy is to give methadone only to palliativ patients, advanced – ususally stage IV – cancer patients that have pain.
I do not “sell” any “miracles”, I give the patients an objective teaching what to expect: side effects, dangers of opioid use – most of them though are already on opioids and thus have already the opioid side effects, so I just have to switch them over to methadone and I am astonished how quick the mental state of the patients turn much better on methadone compared to Hydromorphone which is the standard pain treatment in Austria, due to the additional Endorphinic action of methadone.
As a physician with diploma in palliative medicine I have been tought of cycling opioids and have the licence to do so, and the Austrian medical chambers president confirmed that I can do so.
Still most of the oncologist here act as if exchanging their Hydromorphone to Methadone would be a severe medical fraud that needs to be forbidden with every means. Strange world ?!
Maybe its the price: 2 months of treatment is about 15,-
How to start if opioid native
never start higher as 2 x 5 drops of the 1% racemat solution. Never increase more than 2 x 1 drops a day. Give the patients time to get adjusted to the opioid: if side effects get stronger (tiredness, dizzyness, nausea) then reduce dose for some days befor escalation again. For Nausea use metoclopramide, for constipation the regular stuff,e.g. macrogol or whatever.
The best endorphine action is reached with 2 x 17 drops, the best chemo-adjuvation with 2 x 30-35 drops. Lower doses also help
Resources
there are many resources in german language, e.g. my homepage. TV-Documentations, Journal PDFs …
{kind=link}